
 Processed and ultra-processed food and risk of Inflammatory Bowel Disease in the European Prospective Investigation into Cancer and Nutrition cohort (EPIC-IBD)7th D-ECCO WorkshopPyroptosis Inhibition Prevents the Cytotoxicity Induced by IL-17 Without Impairing Its Beneficial EffectsECCO'22 VirtualRapidity of ozanimod-induced symptomatic response and remission in patients with moderately to severely active Ulcerative Colitis: Results from the induction period of True NorthECCO'22 Virtual
Processed and ultra-processed food and risk of Inflammatory Bowel Disease in the European Prospective Investigation into Cancer and Nutrition cohort (EPIC-IBD)7th D-ECCO WorkshopPyroptosis Inhibition Prevents the Cytotoxicity Induced by IL-17 Without Impairing Its Beneficial EffectsECCO'22 VirtualRapidity of ozanimod-induced symptomatic response and remission in patients with moderately to severely active Ulcerative Colitis: Results from the induction period of True NorthECCO'22 VirtualOzanimod, a sphingosine 1-phosphate (S1P) receptor modulator selectively targeting S1P1 and S1P5, is approved in the US for the treatment of moderately to severely active ulcerative colitis (UC). In the pivotal phase 3 True North randomised controlled trial in moderate-to-severe UC, significantly more patients (pts) achieved clinical response and remission with ozanimod vs placebo (PBO) at week (wk) 10 of the induction period. Here, we report the rapidity of ozanimod-induced symptomatic response and remission in pts from True North (NCT02435992).
MethodsIn True North, pts were randomised to once-daily ozanimod 0.92 mg (equivalent to ozanimod HCl 1 mg) or PBO (Cohort 1) or received open-label ozanimod (Cohort 2) during induction. This analysis evaluated symptomatic response (defined as ≥1 point and ≥30% decrease from baseline in adapted partial Mayo score and ≥1 point decrease from baseline in rectal bleeding score [RBS] or absolute RBS ≤1) and symptomatic remission (defined as RBS of 0 and stool frequency score [SFS] ≤1 point and ≥1 point decrease from baseline at each study visit from wk 2 through 10.
ResultsDuring induction, 645 pts were randomised to ozanimod (n=429) or PBO (n=216) in Cohort 1, and 367 pts received open-label ozanimod in Cohort 2. Baseline demographics and clinical characteristics were well balanced across groups. Differences in symptomatic response were observed between ozanimod and PBO recipients in Cohort 1 as early as 2 wk after ozanimod initiation (1 wk post-titration) for the overall population (36.1% vs 26.4%; difference: 9.6% [95% CI, 2.1–17.0]; Figure 1) and tumour necrosis factor inhibitor (TNFi)-naïve pts (38.5%, n=301 vs 29.1%, n=151; difference: 9.4% [95% CI, 0.2–18.5]), and as early as 4 wk for TNFi-exposed pts (42.2%, n=128 vs 27.7%, n=65; difference: 15.8% [95% CI, 1.8–29.8]). Differences in symptomatic remission were observed between ozanimod and PBO recipients in Cohort 1 as early as 5 wk after ozanimod initiation (4 wk post-titration) for the overall population (26.3% vs 16.7%; difference: 8.6% [95% CI, 1.8–15.4] Figure 2), as early as 4 wk for TNFi-naïve pts (27.2% vs 17.9%; difference: 9.4% [95% CI, 1.5–17.4]), and as early as 8 wk for TNFi-exposed pts (22.7% vs 12.3%; difference: 11.7% [95% CI, 1.3–22.1]). Rates of symptomatic response and remission in pts receiving open-label ozanimod (Cohort 2) were similar to those in pts receiving randomised ozanimod (Cohort 1).
ConclusionIn the overall population, ozanimod was associated with higher rates of symptomatic response and remission vs PBO as early as 2 and 5 wk, respectively, after treatment initiation. Both clinical endpoints were more rapidly achieved in TNFi-naïve vs TNFi-exposed pts.

Real World Effectiveness, Safety and Pharmacokinetics of Switching Intravenous Vedolizumab Maintenance treatment to Subcutaneous Vedolizumab Therapy for Inflammatory Bowel DiseaseECCO'22 VirtualSubcutaneous (SC) formulation of vedolizumab (VDZ) is available for Crohn’s disease (CD) and ulcerative colitis (UC). We assessed the efficacy, safety, and pharmacokinetic (PK) profiles of patients with inflammatory bowel diseases (IBD) who switched from intravenous (IV) to SC VDZ treatment in two prospective, real world cohorts.
The primary cohort is an ongoing open-label, real life, prospective single centre cohort study. As a validation cohort, we used the Initiative on Crohn and Colitis (ICC) registry, a prospective, observational, nationwide registry including patients switching from IV to SC VDZ. In both cohorts, patients receiving IV VDZ maintenance for >4 months were offered to switch treatment to SC VDZ, 108 mg every 2 weeks. In the primary cohort, assessment of clinical, biochemical and PK parameters took place at baseline, at approximately 10 weeks following the switch and at the physician’s discretion thereafter. In the ICC cohort, follow up visits were at week 12 and 24. The primary endpoint was the proportion of patients discontinuing SC VDZ at week 24.
ResultsIn total, 78 (50 CD (64%) and 28 UC (36%)) and 54 patients (29 CD (54%) and 25 UC (46%)) were included in the primary and ICC cohort respectively (table 1). During follow up, 8 (10.3%) of the primary cohort and 6 (11.1%) patients of the ICC cohort stopped VDZ SC during follow-up time till week 24, after a median treatment duration of 18 (IQR=5-19) and 10 (IQR=7-15) weeks, respectively. Treatment withdrawal was most often caused by adverse events (AE), in total for 8 out of 132 patients (6%) (table 2). Four patients had loss of response to SC VDZ. Three of these patients had biochemical disease activity at initiation of SC therapy. Reported AEs included headache and injection related reactions. The median VDZ concentration increased from 11 ug/mL (IQR=9.4-20) to 28 ug/mL (IQR=24.3-31.2, p<0.0001) and from 20 ug/mL (14.3-26.3) to 34.6 ug/mL (26.8-42.9) (p<0.01), between baseline and visit 1 in the primary and validation cohort, respectively (figure 1).

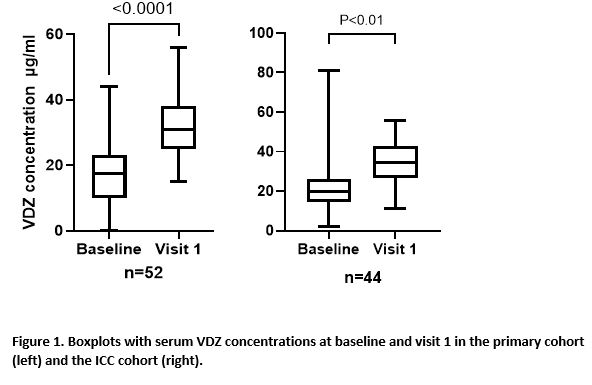

The present abstract reports real world experience of switching IV to SC VDZ maintenance treatment in IBD patients in two observational Dutch cohorts. VDZ concentrations were significantly higher after the switch to SC VDZ. A switch from IV to SC VDZ appears to be effective and safe. However, a proportion of patients switched back to IV VDZ due to injection related AEs.
Real-world multicenter comparison of effectiveness between tofacitinib and vedolizumab in patients with Ulcerative Colitis after failure to at least one anti-TNF agentECCO'22 VirtualRemote monitoring of IBD patients - challenges and future perspectives (Tandem talk)8th ClinCom Workshop