
 Pathogenic RIPK1 Mutations Cause Infantile-onset IBD with Inflammatory and Fistulizing FeaturesECCO'22 VirtualPatients with moderate to severe Crohn’s Disease with and without prior biologic failure demonstrate improved endoscopic outcomes with risankizumab: Results from phase 3 induction and maintenance trialsECCO'22 Virtual
Pathogenic RIPK1 Mutations Cause Infantile-onset IBD with Inflammatory and Fistulizing FeaturesECCO'22 VirtualPatients with moderate to severe Crohn’s Disease with and without prior biologic failure demonstrate improved endoscopic outcomes with risankizumab: Results from phase 3 induction and maintenance trialsECCO'22 VirtualRisankizumab (RZB), a selective interleukin-23 inhibitor, demonstrated clinically meaningful improvements in endoscopic outcomes in patients with moderate to severe Crohn’s disease (CD) during two phase 3 induction trials (ADVANCE and MOTIVATE) and the maintenance study (FORTIFY). Here, we compared the efficacy of RZB in inducing and maintaining improvements in endoscopic outcomes in patients with CD who demonstrated intolerance and/or inadequate response (IR) to biologic therapies (with prior bio-failure) versus those who demonstrated IR to conventional therapies only (without prior bio-failure).
MethodsData included in this subgroup analysis included pooled data from patients randomized to receive intravenous (IV) RZB 600mg (N=527) or placebo (PBO) IV (N=362) every 4 weeks (wks) for 12wks during induction (ADVANCE+MOTIVATE), and data from patients receiving subcutaneous (SC) RZB 360mg (N=141) or withdrawn from RZB IV to receive PBO SC (withdrawal [PBO SC], N=164) every 8wks for 52-wks during maintenance. At Wks 12 and 52, endoscopic response, endoscopic remission, ulcer-free endoscopy (absence of ulceration), and deep remission (Wk52 only) were evaluated both in the overall population and in subpopulations of patients with and without prior bio-failure. (Endpointsare defined in Table footnotes). Safety was assessed throughout the studies.
ResultsApproximately three-quarters of randomized patients included in this subgroup analysis had prior bio-failure (ADVANCE+MOTIVATE: 75.4%; FORTIFY: 73.8%). Higher rates of endoscopic response, endoscopic remission, and ulcer-free endoscopy were observed at Wk12 among patients receiving induction with RZB IV versus PBO IV. Subgroup analysis demonstrated treatment effects with risankizumab in patient subpopulations with and without prior bio-failure, with greater adjusted differences versus PBO in patients without prior bio-failure (Figure). At Wk52, endoscopic response, endoscopic remission, ulcer-free endoscopy, and deep remission rates favored RZB SC compared to withdrawal (PBO SC). Again, treatment effects were observed in patients with and without prior bio-failure, with greater adjusted differences versus withdrawal (PBO SC) in patients without prior bio-failure. RZB maintenance treatment was well-tolerated and no new safety signals were observed. The safety profile of RZB has been reported previously.1,2
Induction and maintenance therapy with risankizumab achieved higher rates for endoscopic endpoints in patients with moderate to severe Crohn’s disease versus placebo, regardless of prior bio-failure status. However, numerically higher efficacy rates were observed in patients without prior bio-failure.
1 D’Haens, G. et al. in DDW 2021 2 Ferrante, M. et al. in UEGW 2021
Perianal fistulas are characterised by expansion of interleukin-22 producing invariant natural killer T-cells and CD4+ T-cells which drive dysregulation of the extracellular matrixECCO'22 VirtualPeripheral blood DNA methylation biomarkers accurately predict clinical- and endoscopic response to vedolizumab in a real-life cohort of Crohn’s Disease patientsECCO'22 VirtualDespite the proven efficacy of vedolizumab (VDZ), only 29% and 36% of the Crohn’s disease (CD) patients present corticosteroid-free clinical- and endoscopic remission, respectively. Therefore, predictive biomarkers for treatment success would be of extreme value. Previous studies have identified aberrant DNA methylation associated with CD-specific phenotypes, suggesting that the methylome may be useful for classification and prediction of VDZ treatment response. Here, we sought to identify such DNA methylation biomarkers that can predict clinical- and endoscopic response to VDZ in CD patients.
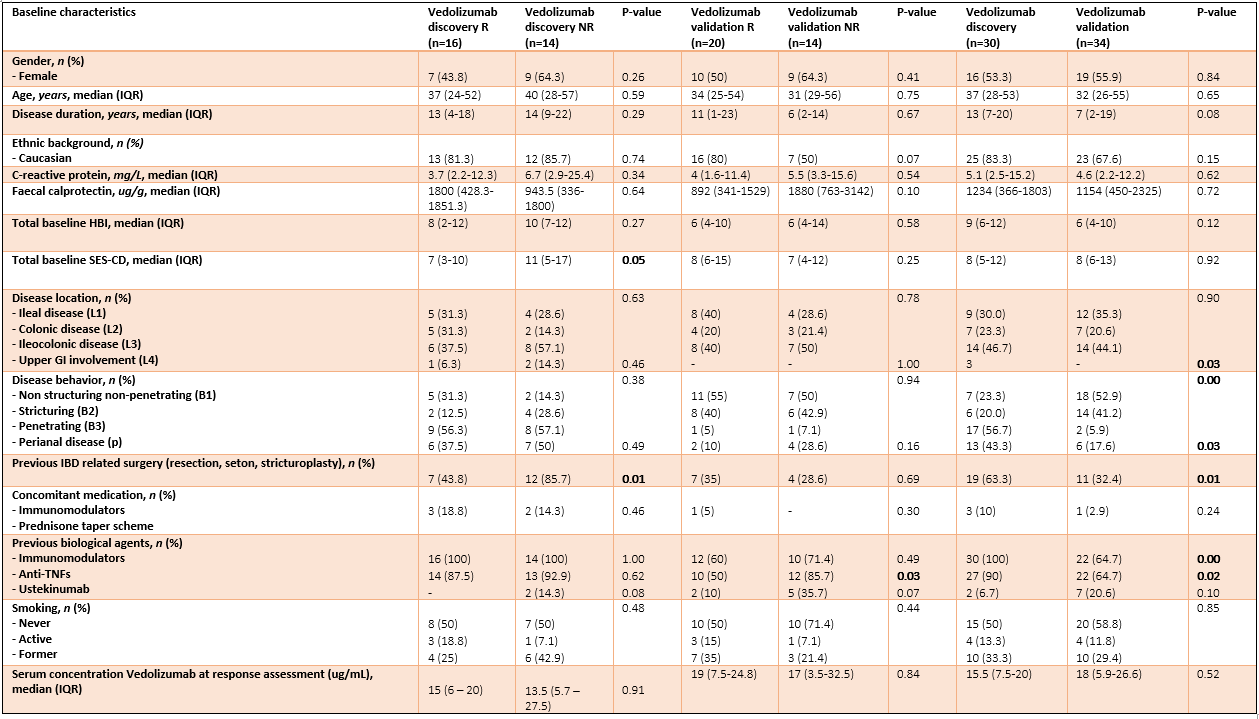
MethodsWe prospectively recruited adult CD patients that initiated VDZ treatment following a baseline colonoscopy in two cohorts: a discovery and validation cohort. Peripheral blood DNA methylation profiles were measured prior to treatment (T1), and after a median of 22 weeks (T2) using the Illumina Infinium HumanMethylation EPIC BeadChip array. Response (R) was defined as the strict combination of endoscopic- (≥50% reduction in SES-CD score) and steroid-free clinical response (≥3 point drop in HBI and HBI ≤4 AND no systemic steroids) and/or biochemical response (≥50% reduction in C-reactive protein (CRP) and fecal calprotectin or a CRP ≤5 g/mL and fecal calprotectin ≤250 µg/g). Twenty-one patients had deep remission (DR), defined as a combined endoscopic- (SES-CD≤2) and steroid-free clinical remission (HBI ≤4, no systemic steroids). Biomarker identification and classification analyses were performed using stability selection gradient boosting.
ResultsIn total, 64 CD patients were enrolled (discovery 16R/14NR and validation 20R/14NR). Both cohorts were comparable for age, sex and smoking status. Forty-nine (77%) patients had previously failed an anti-TNF agent. All patients had measurable serum vedolizumab concentration at T2 (median 14.5 (6.9 – 21.3) µg/mL). Through classification analysis at T1, we were capable of discriminating R from NR with high predictive performance (25 CpGs, AUC 0.88, F1-score of 0.84, PPV of 0.91 and NPV of 0.85). When analysing the methylome of patients in deep remission, we identified 23 CpGs with high predictive performance upon independent validation (F1-score 0.80, PPV of 0.71 and NPV of 0.86). Investigating the CpGs of interest implicated genes involved in endothelial cell-cell adhesion and integrin dependent T-cell homing, corroborating VDZ’s mode of action.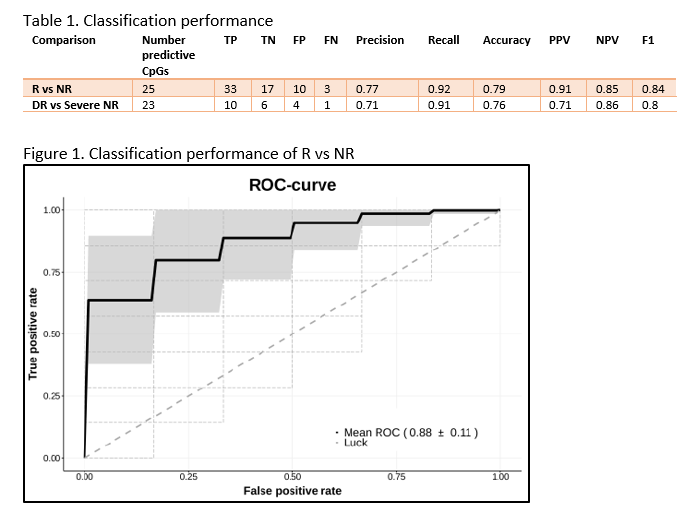
We demonstrate two novel 25- and 23-feature panels of epigenetic biomarkers that accurately predict response or deep remission to vedolizumab respectively. Similar analyses on infliximab, adalimumab and ustekinumab are currently ongoing as part of the EPIC-CD study.
Phenotypic and genetic determinants of medication response in patients in the UK IBD BioResourceECCO'22 VirtualInflammatory bowel disease (IBD) exhibits heterogeneity at genetic, phenotypic, and therapeutic levels [1]. Although several studies have investigated genetic effects on IBD subtypes and drug adverse events [2,3], few have comprehensively explored the phenotypic and genetic determinants of IBD drug efficacy in a sufficiently powered cohort.
MethodsWe used data from 32,199 patients in the UK IBD BioResource to investigate the effects of clinical phenotypes and demographics on drug efficacy and combined this with genome-wide genetic data for a subset of 11,536 individuals (Table 1). Drug efficacy was defined using a combination of clinician reported efficacy and persistence on drug without treatment escalation. Anti-TNF, thiopurine, steroids, and mesalazine were explored. We estimated phenotypic effects on drug efficacy using multivariable logistic regression and the genetic effects by genome-wide logistic regression. To explore whether drug efficacy and IBD disease susceptibility share a genetic basis, we estimated the proportion of variance in drug efficacy explained by known IBD risk variants [4]. Associations with Bonferroni corrected P-values < 0.05 were defined as statistically significant in phenotypic analyses and a genome-wide significance threshold of P=5x10-8 was adopted for genetic analyses.
ResultsDrug efficacy was generally lower in patients with Crohn’s disease (CD) compared to those with other subtypes (OR ranges from 0.40 to 0.79), but anti-TNF showed a higher efficacy rate (OR = 1.21) in CD patients. Increasing age at diagnosis was associated with evidence of increased efficacy of thiopurine and mesalazine (Table 2). We found evidence of a genetic contribution to variation in drug efficacy for most drugs studied. However, known IBD risk variants showed little contribution (Figure 1). Using genome-wide association testing, we identified three loci showing a significant association with drug efficacy; two were related to steroid response and one to thiopurines (Table 3). None of these was an IBD disease susceptibility locus (P > 0.05).
ConclusionUsing a large, well-characterised cohort we found both genetic and phenotypic determinants of drug efficacy. Three loci were reported to be associated with drug efficacy in the first phase of the genetic analysis; at least 4,200 extra genotyped samples will be included before the ECCO meeting, thus increasing the power to detect additional loci. Our results suggest the genetic causes of drug efficacy and disease susceptibility are largely independent. These findings may provide opportunities for exploring the biology of drug efficacy and improving medication prioritization in IBD patients.
Reference
1. PMID: 16819502
2. PMID: 26490195
3. PMID: 30806694
4. PMID: 28067908



Postoperative complications and disease recurrence after surgery for Crohn's disease11th S-ECCO IBD MasterclassPotential mechanisms linking biological therapies on SARS-CoV-2 susceptibility in Inflammatory Bowel Disease patientsECCO'22 VirtualPredicting response to medications in IBD - From basic science to practical approachECCO'22 VirtualProactive Therapeutic Drug Monitoring is superior to standard treatment during maintenance therapy with infliximab; results from a 52-week multicentre randomised trial of 450 patients; the NOR-DRUM B studyECCO'22 VirtualProactive therapeutic drug monitoring (TDM), individualized treatment based on scheduled assessments of serum drug levels, has been proposed to optimize efficacy and safety of infliximab and other biologic drugs. However, it is unclear whether this strategy improves clinical outcomes.
MethodsIn this 52-week randomised, open-label, multicenter trial, adult patients with an established diagnosis of ulcerative colitis (UC), Crohn’s disease (CD), rheumatoid arthritis (RA), spondyloarthritis (SpA), psoriatic arthritis (PsA), and psoriasis (Ps) receiving infliximab therapy for a minimum of 30 weeks were randomly assigned to proactive TDM or standard infliximab treatment. In the TDM group, infliximab dosage was adjusted according to an algorithm designed to maintain serum infliximab levels within the therapeutic range 3-8 mg/L. In the standard treatment group, infliximab dosage was based on clinical judgement.The primary endpoint was sustained disease control during the 52 week study period.
ResultsIn total, 458 patients were randomised of whom 454 (UC 81, CD 66, RA 79, PsA 53, SpA 138, Ps 37) received the allocated strategy and were included in the primary analyses. The two groups were balanced regarding baseline demographics, clinical and treatment characteristics. Sustained disease control without disease worsening was observed in 167 (73.6 %) patients in the TDM group and in 127 (55.9%) patients in the standard treatment group. The estimated adjusted difference was 17.6% (95% confidence interval (CI), 9.0-26.2, p<0.001), favouring TDM (figure 1). Results were consistent in sensitivity analyses. Time to disease worsening was shorter in the standard treatment group, hazard ratio 2.1 (95% CI 1.5-2.9) (figure 2). Other secondary endpoints reflecting change in disease activity and patient reported outcomes from baseline to week 52 did not show significant differences between the two groups. During the trial, the mean infliximab dose (4.8 mg/kg) and median serum level of infliximab (5.8 mg/L) were comparable in both groups. Twenty-one (9%) patients in the TDM group and 27 (15%) in the standard treatment group developed clinically significant levels of anti-drug antibodies (≥50µg/L). Adverse events were reported in 137 (60%) and 142 (63%) patients in the TDM and standard treatment groups, respectively.
Figure 1

Figure 2
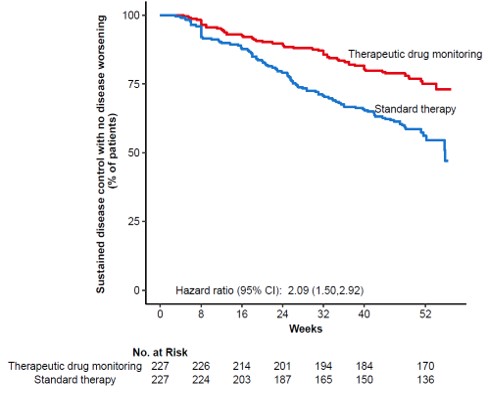
This large randomised controlled trial demonstrates that proactive TDM is superior to standard treatment for maintaining disease control without disease worsening in patients on maintenance therapy with infliximab. These results support implementation of proactive TDM as a general strategy during maintenance therapy with infliximab and have the potential to change clinical practice across specialities.